
Conditons and Surgical Treatments
Shoulder
Arthritis
What are the symptoms of shoulder arthritis?
- Pain – which is aggravated by activity and progressively worsens
- A deep, aching pain in the joint
- Soreness to touch the joint
- Difficulty lifting arms to comb hair or reach to a shelf
- Click and grinding sounds may also be noticeable as you move your shoulder
- Difficulty sleeping due to shoulder pain
- If the glenohumeral shoulder joint is affected, the pain is centered in the back of the shoulder and may intensify with changes in the weather.
- Arthritis relating to the acromioclavicular (AC) joint is focused on the top of the shoulder and this pain can sometimes travel to the side of the neck.
- Someone with rheumatoid arthritis may have pain throughout the shoulder if both the glenohumeral and AC joints are affected.
- Someone with osteoarthritis may have pain throughout the shoulder if both the glenohumeral and AC joints are affected.
What are surgical treatments?
- If non-surgical treatments such as cortisone, physiotherapy and medication do not relieve pain surgical treatments may be very helpful in reducing pain, improving sleep and helping you return to everyday activities.
- Advanced arthritis of the shoulder can be treated with a shoulder replacement (arthroplasty).
- In this procedure, the damaged parts of the shoulder joint are removed and replaced with artificial components called prostheses.
What are the different types of shoulder replacements?
- Although shoulder replacements aren’t as common as hip or knee replacements, they offer the same success in returning function and relieving pain.
Total shoulder replacement
- In total shoulder replacement, the damaged bone of the humerus and of the glenoid are replaced with metal and poly replacement components.
Reverse Total Shoulder Replacement
- Some patients with shoulder arthritis are diagnosed with a special type of shoulder arthritis called cuff tear arthropathy. Patients with cuff tear arthropathy will not benefit greatly from a total shoulder replacement because the cuff is a very important part of being able to lift the arm. Alternatively, a reverse total shoulder replacement changes the anatomy of the shoulder such that the deltoid muscle can function without a rotator cuff muscle, allowing the patient to lift their arm pain free.
- In all, reverse total shoulder replacements are becoming a more popular choice of shoulder replacement for all shoulder arthritis conditions.
Mathys Short Stem Total Shoulder Replacement
- The critical factors when looking at shoulder replacement are stability and function. The shoulder is not a weight bearing joint like the knee and so different considerations are important.
- This option is best suited for younger patients. The Mathy’s short stem shoulder replacement is bone preserving and has a variable angle interface to maximise and restore biomechanical function.
Personalised Reverse and Total Shoulder Replacement
- The shoulder is not a weight bearing joint like the knee and so different considerations are important. Best suited for patients with abnormal anatomy, patient specific instrument technology (PSI) is tailor made for your joint, rather than a one-size-fits-all approach – giving you maximum stability from your prothesis placement. This condition is also multi-purpose and addresses both rotator cuff tears AND arthritis.
Arthroscopy
What is Arthroscopy?
- Also called key hole or minimally invasive surgery, arthroscopic surgery is a simple day stay procedure which involves Dr Herald using a special instrument known as an arthroscope.
- The arthroscope allows Dr Herald to look into your joint (shoulder, elbow or knee) via a very small incision (usually less than 1cm) without having to open the joint up.
- With fibre-optic light and a magnifying glass, the arthroscope provides a very accurate view of your joint to determine what needs a clean up, repair or reconstruction.
- A miniscule camera simultaneously transmits images of your joint to a TV monitor for Dr Herald to view.
What conditions is arthroscopy used to diagnose and treat?
Arthroscopy is useful for many acute sports and work injuries including
- Shoulder Arthritis
- Shoulder Instability
- Shoulder stiffness
- Subacromial Decompression (shoulder impingement)
- Frozen Shoulder
- Removal of loose bodies floating around the joint
What are the benefits?
- Day surgery, so there’s no need to stay in hospital for lengthy periods
- Optimal recovery due to less invasive procedures
- Less risk of infection or after care issues
Burners and Stingers
What are the symptoms?
- Burners and Stingers are terms used to impact injuries to nerve tissue and commonly occur when the shoulder is hit with an elevated arm.
- They describe the type of pain that is experienced at the time of impact which may spread form the site of impact on the shoulder along the entire length of the nerve to the fingers.
- Burners and stingers often happen in contact sports where they may also be called a “dead arm”.
What is the treatment?
- Like a temporary bruise, treatment usually involves rest or gentle range of motion (ROM) exercises until the nerve recovers. Over the counter medications can be used for pain relief or anti-inflammation medication for more persistent injury.
Emergency and Sporting Injuries
- During these matches, acute first aid treatment is usually performed by onsite physiotherapists or by a nearby hospital emergency department or a GP.
- Injuries are usually splinted using a sling and it is important to reduce swelling with ice and elevation where possible.
- Once imaging has been performed definitive treatment can be decided on the sooner the better. The treatment may be non-surgical or surgical.
SLAP lesions are common in overhead throwing athletes and are difficult to diagnose. If you have symptoms with throwing and all previous tests are normal you may require an MR Arthrogram to diagnose the problem.
Fractures
- They can occur as a result of a high-energy injury in a strong bone or a low energy injury in weak bone.
- Initial first aid treatment includes pain relief and a sling to rest the shoulder.
- Ice and compression should be used to reduce the swelling and imaging performed to decide on treatment.
- Most injuries can be treated conservatively with a sling and some physiotherapy usually for around 2 months.
- Sometimes, due to deformity or poor healing, surgery is needed to reduce the fractured bone fragments and secure them to allow early movement.
- It is important that early movement occurs after surgery or injury as otherwise the development of a frozen shoulder can occur.
Collarbone fracture (clavicle)
- A clavicle fracture is also known as a broken collar bone. Broken collar bones are very common and are usually caused by a direct blow to the bone itself or from falling on an outstretched arm.
- X-ray will confirm severity of the break. Non-displaced fractures can heal without surgery, whereas displaced fractures typically require surgery.
Scapula or Shoulder Blade fractures
- Shoulder blade fractures are very uncommon. Typically shoulder blade fractures occur in the lower or inferior aspect of the bone.
- Many of these fractures can be treated without surgery. Symptoms include extreme pain and swelling close to the site of injury.
Upper Arm or Proximal Humerus Fracture
- These kind of fractures frequently occur in elderly people when there is a fall from an outstretched arm.
- A fall can be a simple fall from standing in the elderly to a more vigorous fall from a bike in a younger person.
- They are commonly seen as osteoporotic or weak bone injuries in older people.
What is the treatment?
- While many proximal humeral fractures may no need surgery, they can be very dangerous due to the risk of cutting the nerve and blood supply which runs along the humerus to the hand.
- It is always best to get the right advice for your proximal humeral fracture.
Frozen Shoulder
Frozen shoulder (adhesive capsulitis) is a painful stiffness of the shoulder that often occurs between the ages of 40 and 60 and is more common in women.
Symptoms of frozen shoulder include:
- Pain and stiffness that makes it difficult to carry out a full range of normal shoulder movements such as bathing, dressing, driving and sleeping comfortably.
- Symptoms vary from mild to severe where it may not be possible to move the shoulder at all.
- It may be a self-limiting condition often resolving or “thawing” out, over a 2 year period.
What are the signs that I might need surgery?
Persistent pain that does not go away needs assessment. Remember, either shoulder can be affected, in many cases the non-dominant shoulder (eg the right shoulder in a left-handed person).
In about 20 per cent of cases the condition also develops in the other shoulder.
People with diabetes and thyroid conditions are thought more likely to develop frozen shoulder.
What does surgery involve?
Once a diagnosis has been made, (and if the pain is severe and prolonged), your surgeon may recommend an arthroscopic capsular release to speed up recovery.
During this procedure, the scarred capsule is divided or released to allow full shoulder movement.
Although this is a day surgical procedure, there is usually a 6-12-week period of physiotherapy required afterwards to ensure it does not refreeze.
Dr Jonathan Herald assesses and treats frozen shoulder (both non-surgically and surgically).
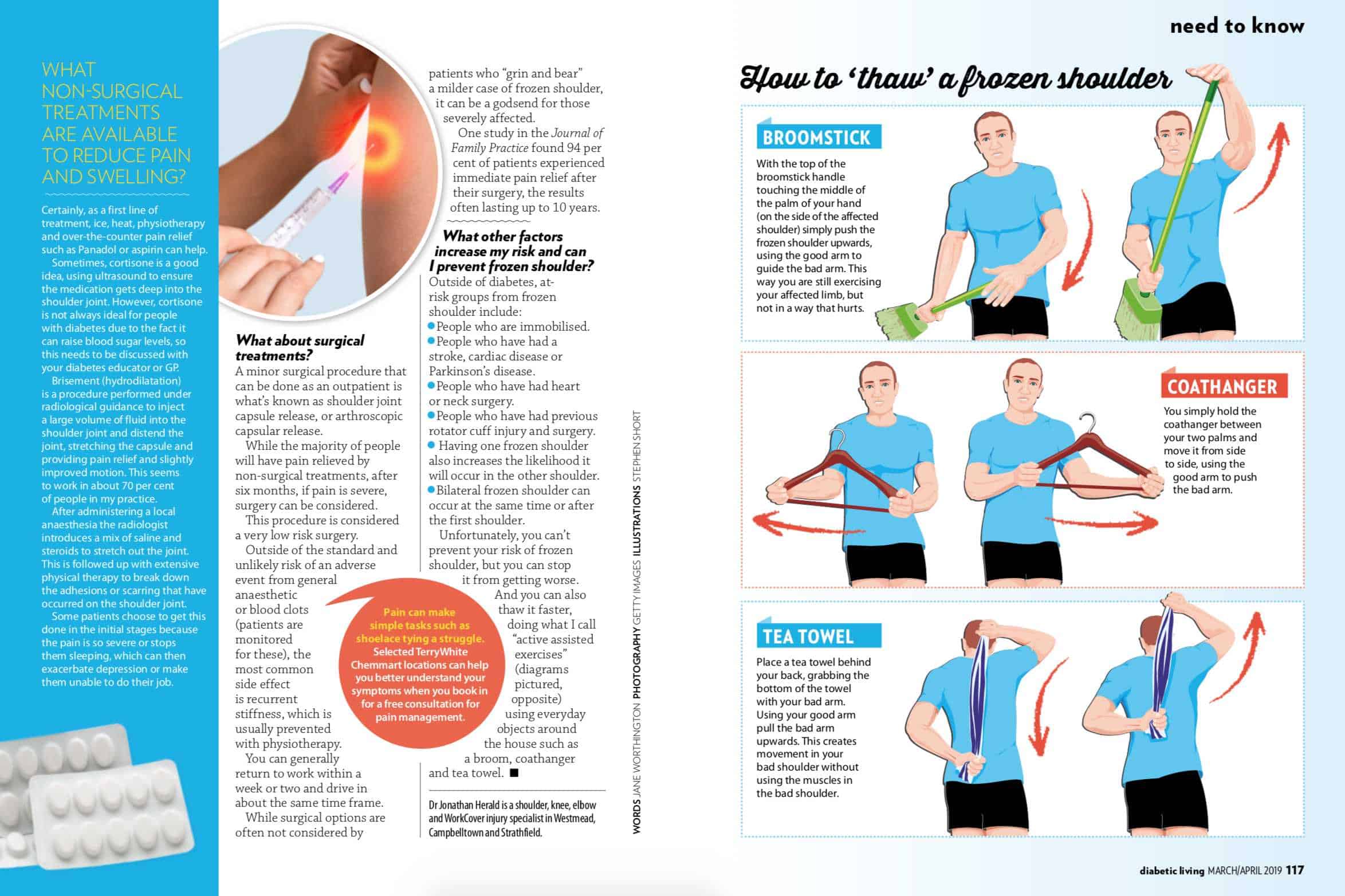
His active assisted exercises for patients to do at home to help thaw a frozen shoulder are here and here. Dr Herald does not perform cortisone injections but can advise whether they are suitable or not for you and refer on.
{kind=link}
He can also advise on best practice rehab advice for frozen shoulder and has physios on site in city rooms.
Rotator Cuff and Other Tears
- Swelling and pain in the front of the shoulder and side of the arm
- Pain felt when raising or lowering the arm
- A clicking sound when raising the arm
- Stiffness
- Pain that causes you to wake from sleep
- Pain when reaching behind the back
What is the treatment?
- Steroid injections, anti-inflammatory medication and physical therapy may all be useful in the treatment of rotator cuff tears. Even though most tears cannot heal on their own, good function can often be achieved without surgery.
- If, however, you are active and use your arm for overhead work or sports or have pain, then surgery is usually recommended because many tears will not heal without surgery and may get larger with time. Surgery is generally recommended if you have persistent pain or weakness in your shoulder that does not improve after several months of non-surgical treatments.
- Surgery is also generally recommended when the tear is large (more than 3cm) and often recommended when the tear is caused by a recent, acute injury or getting larger on serial scans.
What does surgery involve?
- During a rotator cuff repair, the tendon is reattached to the tuberosity bone of the humerus from which it has been torn. This is done using suture anchors in minimally invasive, arthroscopic fashion.
- Bone spurs can also be removed in a similar fashion to prevent further tendon injury. Being a completely arthroscopic surgery, rotator cuff repair surgery is now a more minor procedure than it used to be and is often done as a day surgical procedure.
- The recovery however, still often requires a sling for 6 weeks to protect the repair until it heals.
Other Shoulder Tears
Labral Tears
A shoulder joint labral tear is an injury to the labrum of the shoulder, or to the fibrous ring surrounding the glenoid or socket of the shoulder. When the labrum (made of fibrous cartilage tissue) is torn, it can make the shoulder unstable and cause the shoulder to dislocate. Labral tears are often caused by:
- Falling on an outstretched arm
- Falling on a shoulder
- Bracing with your outstretched arm in a car accident
- Lifting heavy objects repeatedly or too suddenly
- Doing a lot of overhead activities, such as throwing a baseball
There are several different types of labral tears:
- A labral tear above the middle of the socket is called a SLAP Tear. Slap tears occur at the top of the shoulder (11 o’clock to 1 o’clock).
- If the tear is at the front of the shoulder, it is called a Bankart Tear (3 o’clock to 6 o’clock)
- When the tear is at the back of the shoulder (6 o’clock to 11 o’clock it is known as a Reverse Bankart Tear
- Sometimes tears occur in combination and these tears are called 270 degree tears.
What are the symptoms?
- Pain with overhead movements like throwing a ball
- Popping, clicking, or catching in the shoulder
- Pain when you move your arm over your head or throw a ball
- Weakness or instability in the shoulder
- People often have a hard time describing or pinpointing where the pain is or describe it as an “aching” pain.
What is the treatment?
- Usually, a significant labral shoulder tear will need surgery for the best outcome and function. This is generally done via a minimally invasive procedure known as arthroscopy, which can be done as a day surgery. Physiotherapy will be required post surgery.
Biceps Tendon Tear at the Shoulder
What is it?
- The biceps muscle has two tendons at the shoulder; a long head and a short head. At the distal end there is one tendon which crosses the elbow. The biceps muscles allow you to bend the elbow and pronate (rotate) the arm.
- At the shoulder, the long head biceps tendon attaches to the top of the shoulder socket, and the short head biceps tendon attaches to the coracoid process.
- Proximal biceps tendon tears can be partial or complete and most often associated with incomplete tears of the long head of biceps tendon.
- A complete rupture will result in a “Popeye Deformity” where the bicep bunches up and bulges out like Popeye’s arms.
What are the symptoms?
- Popping sounds at injury
- Pain, tenderness and weakness at the shoulder or elbow
- Trouble turning the palms face up or face down
- Bruising
- Bulging above the elbow
- Sharp and sudden upper arm pain
What is the treatment?
- While you may be able to live with a Popeye deformity of a proximal biceps tendon tear, a distal biceps tendon tear needs prompt treatment as the distal biceps tendon can retract from the bone and cannot heal itself.
- Permanent weakness can occur if the tendon is not repaired surgically and a deformed and high riding biceps muscle can cause you to lose more than half of your elbow strength.
- For these reasons, surgical repair is most effective within first two weeks of symptoms. There is about a 3 month recovery post surgery.
Unstable/Dislocating Shoulders
- Our shoulders are the most mobile joint in the body, and any disturbance to the normal anatomy of the shoulder structure can cause shoulder instability which increases risk of dislocation.
- Previous dislocations can make a shoulder feel unstable
- Athletes are also highly prone to this injury (particularly in sports like baseball, swimming and volleyball)
- People who are double jointed are more likely to have this condition, due to looseness in the joint
What are the symptoms?
- Pain caused by shoulder injury
- The shoulder joint feeling “loose” as if the ball is falling out of the socket
- Repeated shoulder dislocations
- Repeated instances of the shoulder giving out
What if it becomes “chronic”?
Once a shoulder has been injured by dislocation, it is highly vulnerable to repeat episodes. When a shoulder has dislocated multiple times it becomes loose and may dislocate spontaneously.
What is the treatment?
- The good news is that this condition can frequently be treated with Arthroscopy – a minimally invasive day procedure.
- Surgical stabilisation (via arthroscopy) involves repairing the torn ligaments.
- As it is usually a day surgical procedure – today it is considered a significantly more minor procedure than it used to be.
- The recovery however still often requires a sling for 6 weeks to protect the repair until it heals.
Dislocated Shoulder
What is a dislocated shoulder?
- The shoulder is a ball and socket joint and is the most mobile joint in the body. But for every advantage the shoulder gains in mobility – it loses in stability.
- The shoulder is highly vulnerable to dislocation and this may be described as a partial (subluxed) or complete dislocation and anterior, posterior or multi-directional.
- Shoulders are frequently dislocated when there is instability.
What are the symptoms of shoulder dislocation?
- Swelling or bruising
- A shoulder that is visibly deformed or out of place
- Severe pain
- Inability to move the joint
- When a shoulder dislocates, the ball of the joint (the humerus), falls out of the socket of the joint (the glenoid).
- In some instances of dislocation, the head of the humerus may be fractured by the glenoid as it dislocates. This is known as a Hill-Sachs lesion.
What is the treatment?
- Dislocated shoulders require urgent medical attention and treatment can range from anti-inflammatory treatments, to physiotherapy, splinting and a closed reduction (doctor popping the shoulder back in place) or an open reduction (doctor popping the shoulder back in place during surgery).
- This condition is extremely painful so while you’re waiting for medical attention, don’t move the joint.
- Splint or sling in current position
- Do not try to put the shoulder back in place – which can damage the joint and nerves.
- Ice the shoulder to prevent swelling.
Shoulder Videos
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/bankart-repair”>Bankart Repair</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/biceps-tenodesis”>Biceps Tenodesis</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/distal-clavicle-excision-resection-arthroscopic-technique/”>Distal Clavicle Excision (Resection, Arthroscopic Technique)</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/glenohumeral-debridement”>Glenohumeral Debridement</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/latarjet-procedure-for-shoulder-instability/”>Latarjet Procedure for Shoulder Instability</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/orif-surgery-for-proximal-humerus-fracture/”>ORIF Surgery for Proximal Humerus Fracture</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/reverse-total-shoulder-replacement/”>Reverse Total Shoulder Replacement</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/rotator-cuff-repair-arthroscopic”>Rotator Cuff Repair (Arthroscopic)</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/slap-repair/”>SLAP Repair</a>
<a href=”https://www.orthoclinic.com.au/videos-and-tutorials/total-shoulder-replacement/”>Total Shoulder Replacement</a>
Knees
Arthritis
Symptoms commonly associated with knee osteoarthritis include:
- Pain that increases when you are active, but gets a little better with rest
- Pain that interferes with daily activities
- Swelling and feeling of warmth in the joint
- Worse pain in colder weather
- Stiffness in the knee, especially in the morning or when sitting for a while
- Long-lasting knee inflammation and swelling that doesn’t get better with rest or medications
- In advanced cases, moderate or severe knee pain while resting, day or night
- A bowing in or out of your leg
- Knock knees
- Knee stiffness
How common is knee surgery?
According to the Australia’s National Joint Registry, there has been an 88 per cent increase in knee replacement surgeries between 2003 and 2014 – with more than 54,000 Australians undertaking the procedure in 2014.
What does surgery involve?
- In general, knee replacement surgery consists of replacing the diseased or damaged joint surfaces of the knee with metal and plastic components shaped to allow continued motion of the knee.
- Knee replacements are performed for severe arthritic knees and can be unilateral (one knee) or bilateral (two knees).
- The operation typically involves substantial postoperative pain, and includes vigorous physical rehabilitation.
- The recovery period may be 6 weeks or longer and may involve the use of mobility aids (e.g. walking frames, canes, crutches) to enable the patient’s return to preoperative mobility. Hospital stay is generally about a week. Most patients can safely drive at 6 weeks and gradually increase walking distances in 6 weeks.
What are the specific types of surgical replacement procedures Dr Herald offers?
Unicompartmental Replacement of The Knee
- For osteoarthritis sufferers where the problem is limited to only one side of the knee, a uni compartmental knee replacement is an alternative surgical option to total knee replacement surgery.
- Your orthopaedic surgeon should be consulted to discuss the extent of your arthritis to determine if a uni compartmental knee replacement is right for you.
Total Knee Replacement
- Advanced arthritis of the knee is very painful. When non surgical treatments like medications and gentle exercise no longer manage pain, the total knee replacement surgery is an effective way to relieve pain, correct deformity and improve function of the knee.
- Total knee replacement surgery is also called knee arthroplasty.
- Knee arthroplasty involves implanting new femoral, tibial, tibial insert and patella components into the knee joint. The implants may be cemented or press fit into position.
- The goal of surgery is to balance the knee so that future wear and tear of the new joint occurs as evenly over the new implant surface as possible. Physiotherapy is a very important part of the post op recovery process of total knee replacement surgery.
Biomet PSI Total Knee Replacement
- Whilst your choice of a long lasting total knee replacement prosthesis is important, equally it is important to get the positioning and balance right when putting it in.
- A combination of using the Biomet Vanguard total knee replacement prosthesis and the Signature personalized (PSI) technology, means you get a powerful combination of durability and fit for the maximum possible life of your joint replacement. A joint tailor-made for your body.
What other conditions require a knee replacement?
Knee replacement is also used for other kinds of knee disease such as:
- Rheumatoid arthritis
- Psoriatic arthritis
- A torn meniscus
- Cartilage defects
- Ligament tears
ACL & Ligaments (ACL Reconstruction)
of the knee.
Signs of ACL damage include:
- A loud “pop” or a “popping” sensation in the knee
- Severe pain and inability to continue activity
- Swelling that begins within a few hours
- Loss of range of motion
- A feeling of instability or “giving way” with weight bearing.
What does surgery involve?
Thankfully surgical reconstruction is generally a very successful operation if done before any permanent chondral or meniscal damage occurs (Dr Herald will assess this with examination and imaging).
As ACL generally does not heal, the surgical reconstruction is performed using either the patient’s own tendon (auto graft form hamstring or patella tendon) or that of a cadaver’s (allograft).
The procedure is usually a day surgical procedure but the reconstructed ligament matures over a one year period so return to sport requires intensive rehab.
OTHER LIGAMENT INJURIES
Posterior Cruciate Ligament Injuries
- The PCL is located at the back of the knee and stops the tibia moving backwards. It is less common to injure the PCL than other types of knee ligaments.
- Impact injuries like dash boards of cars hitting the knee or hyper-extension injuries are the typical mechanisms of injury. The PCL injury may be categorised as a grade 1, 2 or 3 injury, where grade 3 is a complete rupture.
- Complete rupture presents with pain, swelling, instability and loss of range of motion. Surgical treatment may be advised if the patient wishes to return to a high level of function.
Collateral Ligament Injuries
- Collateral ligaments of the knee are the ligaments which brace the sides of the knee joint.
- There is the Medial Collateral Ligament (MCL) and the Lateral Collateral Ligament (LCL).
- As with other types of ligament tears, collateral ligament injuries are categorised as a grade 1, 2 or 3 injury, where grade 1 is slightly stretched and grade 3 is a complete tear or rupture.
- The MCL is more frequently damaged than the LCL due it being easier to create a valgus strain versus a varus strain. Pain, swelling and instability are the symptoms and typically immobilisaton without surgery is the recommended treatment.
Combined Knee Ligament Injuries
- Combined knee ligament injuries are complex injuries and an assessment of which ligaments have been affected and the recovery expectation of the patient need to be carefully considered. Multi ligament tears present with pain, swelling and inflammation. Treatment is often surgical and best soon after the injury.
- Arthrofibrosis or scar tissue of the joint is a risk factor to consider for surgery of these conditions.
Arthroscopy
- Arthroscopic knee surgery is generally a day surgery where small keyhole incisions are made in the knee (as opposed to formal, open incisions) which leads to a quicker recovery and less pain.
- Arthroscopy is generally used in evaluating conditions such as torn floating cartilage (meniscus); removing loose bodies (cartilage or bone that has broken off); patellofemoral (knee-cap) disorders, reconstruction of the Anterior Cruciate ligament or to wash out infected knees.
- Physiotherapy is usually required post operatively and recovery takes around a month.
Discoid Meniscus
- A discoid meniscus is an abnormally shaped meniscus in the knee.
- People with discoid meniscus are more prone to injury than those with a normal meniscus.
- Squatting and twisting motions are the typical mechanisms of injury.
- Symptoms are more frequent in the young.
- There are 3 types of discoid meniscus, incomplete, complete and hypermobile wrisberg.
- Meniscal injuries present with pain, stiffness, swelling, catching, locking, and altered range of motion.
- MRI scans can verify meniscal pathology which is best treated surgically.
Fractures
Kneecap fractures
Some kneecap fractures can cause just a tiny crack in the bone, while others may cause the bone to shatter or stick out through the skin. This kind of injury generally results from a fall or blow to the knee.
Symptoms of kneecap fractures include:
- Pain when your knee is touched or when you move your leg
- You have swelling and bruising around your knee
- You are able to straighten your leg but you cannot bend it
- You cannot stand up or put weight on your injured leg
What is the treatment?
- Treatment can be open reduction-internal fixation surgery where Dr Herald puts the broken bones back together with pins, wires and screws – or removes pieces to damaged to repair.
- Alternatively the kneecap can be removed (either part or all of the kneecap).
- After this surgery the knee can still be extended but the extension strength will be weaker.
- Contact sports should be avoided and stationary bikes and non-weight bearing sports are recommended.
Distal Femar (thighbone) fracture of the knee
- Fractures of the top part of the knee are called distal femur fractures.
- They typically occur in the elderly or in high impact injuries such as a car crash.
- Distal femur fractures can be described as transverse (straight across), comminuted (many pieces) or intra-articular (extend into the knee joint).
- Additionally these types of fractures may be open (where the skin is broken), or closed (where the skin is intact).
- Due to the strong musculature around these fractures, it is common for the muscles to shorten and move the bony fragments away from correct alignment.
What are the symptoms?
- Pain with weight bearing
- Swelling and bruising
- Tenderness to touch
- Deformity — the knee may look “out of place” and the leg may appear shorter and crooked.
What is the treatment?
- Surgery is often indicated for distal femur fractures.
Proximal Tibia (below knee) fracture
- Fractures of the bottom part of the knee joint are called proximal tibia fractures. While most of these fractures occur as a result of trauma, they can also occur as a result of stress fracture or compromised bone due to infection, cancer or osteoporosis.
- Fractures of this region are described as transverse, comminuted or intra-articular.
- Intra-articular fractures involve fracture of the tibial plateau, a much softer part of the tibia which sometimes presents as a depression in the bone rather than a fracture.
- Surgical correction and immobilisation are recommended in proximal tibial fractures.
Symptoms of Proximal Tibia (below knee) fracture include:
- Pain upon movement or when bearing weight
- Tenderness
- Limited ability to bend the knee
- Deformity around or below the knee joint
- The foot may be cold and pale (reduced blood supply)
Knee Dislocation (Multi-Ligament Reconstruction)
- Multi-ligament knee injuries or knee dislocations are serious conditions that require immediate hospital assessment.
- These injuries often occur as a result of a high impact injury such as a car accident or fall from a height.
- They can also occur from sports or work injuries and involve multiple major ligaments being injured. If all four major ligaments are injured the knee may be dislocated.
What are the symptoms of dislocation?
- Severe pain
- Severe swelling
- Inability to walk
- The knee feeling unstable, loose and wobbly
What does surgery involve?
- The knee needs to be reduced urgently and checked for vascular or neural damage.
- Often the leg is splinted until swelling has reduced sufficiently to allow major surgery.
- There is no real role for non-operative treatment in this scenario and staged surgeries are often performed to reconstruct the ligaments with a combination of autograft (patient’s own tendon), allograft (tendon from a cadaver) and synthetic grafts (artificial ligaments). Recovery is up to a year long.
Patellofemoral Pain Syndrome (Runner's Knee)
- The patella or the knee cap sits in a groove at the front of the knee and should glide painlessly up and down through your femoral groove.
- However this is not always the case and Patellofemoral Pain Syndrome is one of the most niggling and common knee complaints of both young and old.
- It is generally caused by poor kneecap alignment and instead of gliding, the kneecap maltracks to one side and grates against the femur.
Symptoms of Patellofemoral Pain Syndrome include:
- Pain around the knee. The pain is felt at the front of the knee, around or behind the kneecap (patella).
- The pain comes and goes
- Stairs, squatting, kneeling, hopping, running are often painful
- There may be a grating or grinding feeling or noise when the knee moves
- Sometimes there is fullness or swelling around the patella
- If the groove or the patella is unusually flat the knee cap may be predisposed to dislocating
- Running and jumping sports like netball and football, running, volleyball, skiing and basketball all see a high level of patellofemoral pain
- As the condition progresses the pain may be more noticeable while walking and even at rest
What is the treatment?
- The good news is that the majority of Patellar Pain Syndrome patients will benefit from physiotherapy intervention, (a mcconnell, along with Rest, Ice and Protection or taping))
- Aim to stay away from kneeling and sporting activities until the knee pain is gone
- Apply ice every 20 minutes for several hours at the onset of pain or if your knee feels warm to the touch
- Speak to your physiotherapist about taping, mobilisation and other treatments along with techniques to improve your kneecap pain.
- Surgery will only be required if there if there is continued maltracking despite an extensive course of physiotherapy..
Patellar Dislocation and Instability in Children
- A child’s kneecap should sit in the middle of the knee in a groove of the femur called the trochlear groove.
- During knee movement, the kneecap should move up and down within the groove.
- When the patella slips out of the groove, it is known as a partial or complete dislocation of the kneecap.
- This is a very painful experience associated with loss of movement, even if the kneecap returns to the groove after it has slipped out.
- If the kneecap remains dislocated the child should be taken to emergency to have it reduced.
- Pain and inflammation should be managed with physiotherapy including immobilisation and VMO quads strengthening.
- Surgical treatment is only necessary if the patient experiences multiple dislocations.
Patellar Instability - (Medial Patellofemoral Ligament Reconstruction)
When the knee is functioning properly, the kneecap runs smoothly in a grove of the femur called the trochlear groove. If the kneecap slides out of this groove, the kneecap will become unstable. Anatomy anomalies like shallow or uneven grooves may cause the kneecap to slide out, or an injury such as a heavy fall or sharp blow to the kneecap may cause it to dislocate. Bracing and strengthening exercises treat minor and single episode dislocations while surgery is advised to correct multiple dislocation injuries.
What does surgery involve?
- Persistent pain should not be ignored as recurrent dislocations can cause damage to the delicate chondral surfaces of the knee joint and predispose to arthritis.
- There are a number of surgical procedures that may help in this situation depending on your anatomy.
- A Medial Patellofemoral Ligament Reconstruction (MPLF) is a surgical procedure indicated in patients with more severe patellar instability.
- An MPFL reconstruction will reconstruct and tighten loose medial ligaments; a lateral release will release tight lateral structures; while a tibial ubercle transfer will realign the whole extensor mechanism by breaking the bone that the patella tendon is attached to and moving it with the patella into a more suitable position.
- Dr Herald will work with you to find the most appropriate surgery and the rehabilitation for you.
Patellar Tendinitis or Tendon Tears
- The patellar tendon is a very strong tendon and resistant to injury.
- Frequent running or jumping can cause a weakening of the tendon via overuse tendinitis or caused by disrupted blood flow to the tendon.
- X-Ray and MRI scans will confirm degeneration and tearing or even a rupture of the patellar tendon, which is best treated by surgical repair.
- Most tendon re-attachments are done as inpatient procedures, however, some treatments for tendinitis such as PRP may be done as outpatient procedures.
- Post-surgery, a combination of knee immobilizer, crutches or walker may be used to prevent you from placing too much weight on the repaired knee.
- Most tendinitis treated early with physiotherapy can avoid surgery.
Meniscal Tear
What are the symptoms of a meniscal tear?
- Pain especially when twisting or rotating the knee
- Stiffness
- Swelling
- Catching
- Locking
- A popping sensation
- Altered range of motion
- Difficulty straightening the knee fully
- MRI scans can verify meniscal pathology which is best treated by surgical repair.
What is the treatment for meniscal tear?
- Initially, rest your knee, and use crutches to avoid any weight bearing on the joint. Avoid any activities that worsen your knee pain.
- Ice your knee every three to four hours for 30 minutes.
- Compress or wrap the knee in an elastic bandage to reduce inflammation.
- Elevate your knee to reduce swelling
Surgical treatment is usually an day surgery, using minimally invasive techniques.
PSI (Patient Specific Implant)
By using preoperative CT scans to create a prosthetic module that fits your knee, we can use technology to create a tailor-made cutting jig – that helps accurately implant a prosthesis in the best position for your joint.
Quadriceps Tendon Tear
- The quads tendon sits above the knee, joining the quads muscles to the top of the patella.
- Tears are more common in middle aged populations. The mechanism of injury is an eccentric (lengthening) contraction of the quads resulting in a painful disabling condition.
- Tendon weakness caused by tendinitis or chronic disease will result in higher risk of sustaining a quads tendon tear. Most large quads tendon tears should be treated surgically.
What are the symptoms of a tear?
- A popping or tearing sensation
- Pain and swelling
- Inability to straighten the knee
- An indentation at the top of your kneecap where the tendon tore
- Bruising
- Tenderness
- Cramping
- Your kneecap may droop because the tendon is torn
- Difficulty walking due to the knee buckling or giving way
What is the treatment?
- Small tears may heal with brace immobilization, crutches and physical therapy.
- However most complete tears require surgery to repair the torn tendon. Surgery involves reattaching the torn tendon to the top of the kneecap.
- Results are better if the repair if performed soon after the injury to prevent tendon scarring or the tendon shortening and tightening.
Shin Splints
- The term “shin splints”, refers to pain along the inner edge of the shin bone.
- Shin splints are an over use injury, involving inflammation of the muscles, tendons and bone of the tibia.
- Shin splints occur with a sudden change of frequency and load of exercise.
- Those with poor arch support or flat feet are at higher risk of developing shin splints.
- Shin splints may develop into stress fracture, tendinitis or chronic exertional compartment syndrome. Treatment involves rest from exercise, inflammation management and arch supports for feet. Surgical treatment is not indicated.
Osgood-Schlatter Disease
Osgood-Schlatter disease is an overuse injury of the knee that typically affects children and adolescents experiencing growth spurts. Kids who are involved in running and jumping sports and other activities which involve swift change of direction are more prone. These include soccer, basketball, netball, ballet and football.
What are the symptoms?
- Pain
- Swelling
- Tenderness below the kneecap
- Painful lump below the kneecap
What is the treatment?
- This is usually a resolving condition, and tends to improve when the child’s bones stop growing.
- Treatment includes a course of non steroidal anti inflammatory drugs (NSAIDs).
- In some patients, Osgood-Schlatter’s may last 2-3 years, but in most cases passes at the end of the growth spurt at 14-16 years old.
Knee Videos
Anterior Cruciate Ligament Tear (ACL Tear)
Complex Regional Pain Syndrome (CRPS)
Procedures
ACL Reconstruction with Hamstring
Autologous Chondrocyte Transplantation
Lateral Release and Medial Imbrication
Meniscus Repair (Arthroscopic Technique)
Microfracture Drilling Procedure for Isolated Chondral Defect
Posterior Cruciate Ligament (PCL) Reconstruction
Visco-supplementation for Arthritis of the Knee
Elbows
Arthritis
Typical symptoms of elbow arthritis include:
- Pain – Generally worse as you rotate the forearm.
- As the condition progresses pain interrupts sleep during the night
- Swelling (more common with rheumatoid arthritis)
- Instability of the joint
- Inability to extend or flex the elbow
- Locking and stiffness
What does Elbow Arthroscopic Surgery involve?
- Arthroscopic elbow surgery is designed at improving elbow stiffness and end range pain but not curing arthritis.
- It is a day procedure where Dr Herald can look inside the joint using a small cut with instruments the width of a pencil.
- Spurs and loose bodies are removed and tight adherent capsules are released.
- The benefit of arthroscopic surgery includes a quicker recovery as only small punctures through the skin are used to access the joint as opposed to formal, open incisions.
- Improved elbow range is obtained under anaesthesia but extensive post operative rehabilitation is needed to maintain this.
- Following surgery, a period of continuous elbow range of motion with a continuous passive motion (CPM) machine is required to maintain motion and prevent recurrent scarring.
What does Elbow Replacement Surgery involve?
- Elbow replacement surgery is usually done if your doctor has assessed your elbow as being badly damaged by osteoarthritis or if the pain is persistent and severe and you cannot use your arm.
- Surgery may also be appropriate may for patients with rheumatoid arthritis, a badly broken bone in the upper or lower arm near the elbow, badly damaged or torn elbow tissues, a tumor or a very stiff elbow.
- During a total elbow replacement procedure, the damaged parts of the elbow-hinged joint are removed and replaced with artificial components called prostheses.
- Replacement options include a hemiarthoplasty where part of the joint is replaced not the olecranon (the bony point of the elbow); a total elbow arthroplasty where the end of the humerus and olecranon is replaced with a metal and plastic hinged joint.
- The decision as to which prosthesis is used is dependent on your surgeon, the degree of your arthritis and your age.
- As the elbow is a much smaller joint than a knee or a hip there is generally a 3kg lifting restriction applied following surgery to prevent the plastic wearing out too soon.
Arthroscopy
- Arthroscopic elbow surgery is a day procedure where Dr Herald can look inside the joint using a small cut with instruments the width of a pencil.
- Spurs and loose bodies are removed and tight adherent capsules are released.
- The benefit of arthroscopic surgery includes a quicker recovery as only small punctures through the skin are used to access the joint as opposed to formal, open incisions.
What conditions is elbow arthroscopy useful for?
- Elbow arthroscopy can be useful in diagnosis and treatment of arthritis, loose bodies in the joint, tennis elbow, stiffness and fractures.
What happens after the procedure?
- Improved elbow range is obtained under anaesthesia but extensive post operative rehabilitation is needed to maintain this.
- Following surgery, a period of continuous elbow range of motion with a continuous passive motion (CPM) machine is required to maintain motion and prevent recurrent scarring.
- The CPM machine is used in hospital for around 3 days continuously and for most of the day for up to a month after.
- A physiotherapist is an important part of your post-operative rehabilitation.
Biceps Tear (Distal Biceps Repair)
- The biceps muscle has two tendons which insert into the shoulder.
- These muscles allow you to bend the elbow and rotate the arm.
- A biceps tendon tear at the elbow is generally less common than a biceps tendon tear at the shoulder.
What are the symptoms?
- Popping sounds at injury
- This kind of injury often occurs on heavy lifting
- Pain, tenderness and weakness at the shoulder or elbow
- Trouble turning the palms face up or face down
- Bruising
- Bulging above the elbow
- Sharp and sudden pain near the elbow
What is the treatment?
- A severe biceps tendon tear needs prompt treatment as the distal biceps tendon cannot regrow back to the bone and heal itself.
- Permanent weakness can occur if the tendon is not repaired surgically and a deformed and high riding biceps muscle can cause you to lose more than half of your elbow strength.
- For these reasons, surgical repair is most effective within first two weeks of symptoms.
- There is about a 3 month recovery post surgery.
.
Lateral Epicondylitis (Tennis Elbow)
- Lateral epicondylitis is a painful condition that affects the muscles and tendons of the forearm.
- It is commonly referred to as “tennis elbow” but rarely occurs as a result
of tennis these days.
Symptoms of this condition include:
- Tenderness on the outer bony part of the elbow
- Morning stiffness of the elbow with persistent aching
- Soreness in the forearm
- Pain worse when grasping or holding an object
- The forearm tendons that attach to the outer aspect of the elbow may become inflamed and torn as result of repetitive over extension of the wrist and elbow.
What does surgery involve?
- In most cases, the micro tears and inflammation settle down and heal with rest but in some recalcitrant cases surgery is required.
- This involves repairing the torn extensor tendons after excising the degenerate segment and performing a tendon release.
- Both result in reduced pain and increased grip strength.
- A sling is required for comfort post-operatively and physiotherapy also.
Fractures
What are the symptoms?
- Swelling, bruising and pain
- An audible snap or pop at time of injury
- Visible deformity or banana arm
- Numbness or weakness in the arm, wrist and hand
There are three main type of elbow fractures including:
Head of The Radius Fracture
- This injury usually causes pain with forearm rotation (palms turned up then down again).
- These kind of fractures rarely require surgery to either fix or replace the radial head.
Olcrenon Fracture
- These fractures are often displaced and almost all require surgery.
- The bone fragments are re-aligned and held together with pins and wires or plates and screws.
Distal Humerus Fractures - These fractures occur commonly in children and in the elderly.
- Nerve and/or artery injuries can be associated with these types of fractures. These fractures usually require surgical repair with plates and/or screw, unless they are stable.
Forearm Fractures
- Dr Herald can also treat forearm fractures. There are several types of forearm fractures (sometimes severe breaks are called banana arm).
- Forearm fractures typically account for 4 in 10 childhood fractures.
What are the different types of forearm fractures?
- Torus fractures – In this injury, one side of the bone compresses, causing the other side to bend away from the growth plate. This is a stable fracture, meaning that the broken pieces of bone are still in position and have not separated apart (displaced).
- Buckle Fractures – Also known as Metaphyseal fractures, these breaks frequently affect babies and toddlers. The fracture is across the upper or lower portion of the shaft of the bone and does not affect the growth plate.
- Greenstick fracture. Another fracture of babies and young children, this is where soft bone breaks on one side and bends on the other – the euphemism refers to greenwood which also breaks when bent.
- Galeazzi fracture. This injury affects both bones of the forearm. There is usually a displaced fracture in the radius and a dislocation of the ulna at the wrist.
- Monteggia fracture. This requires urgent medical attention as it is a severe injury. It affects both bones of the forearm – the ulna and the top (head) of the radius is dislocated.
- Growth plate fracture. Because the growth plate helps determine the future length and shape of the mature bone, this type of fracture requires urgent attention. Trauma that would cause a sprain in an adult might actually fracture a growth plate in a child.